Diabetic foot ulcers (DFU) are one of the most serious complications of diabetes and one of the important causes of mortality and morbidity among people with diabetes (Wang et al, 2022; McDermott et al., 2023). The management of DFU remains a critical challenge for healthcare providers.
Current standard treatments often struggle to effectively address the persistent infection and impaired healing characteristic of these wounds. Appropriate treatment of DFU requires a multifaceted strategy that includes timely, correct diagnosis and classification. Multiple assessments of the risk factors and the appropriate choice of management should be based on the patient’s actual condition (Wang et al, 2022; Lee et al, 2024). The ultimate objective of DFU treatment is to achieve healing and prevent wound infection that may result in amputation and reduced quality of life (Yang et al, 2022; Gong et al, 2023).
This case series demonstrated the innovative approach and efficacy of a topical silver nanoparticle-based spray that combines four key agents – silver, chlorhexidine, silicon dioxide and hyaluronic acid (KAdermin YSP, Trident Pharmaceutical Sdn. Bhd.]) – in a powerful wound dressing developed specifically for DFU.
Methods
Study design
Six patients from Wound Care Unit Hospital Tuanku Fauziah, Malaysia, with DFU were enrolled in this case series by convenient sampling. All of them presented with different sizes of wounds were initially treated with other types of dressing before the introduction of KAdermin spray.
Dressing regime
Each patient’s wounds were cleaned with Electrocyn soma (V3bio Sdn. Bhd.) solution. Then, KAdermin spray was applied over the entire wound surface. Wounds then were covered with gause and bandages. This dressings regime was done twice a week for all patients in this case study.
Data collection
Patient data, including age, sex and comorbidities, were taken from the assessment records. Progression of healing was recorded in wound chart by measuring initial wound size before the use of KAdermin spray dressing and final wound size observed at 12 weeks or earlier upon discharged when their wounds healed.
Case presentations
Case 1
A 46-year-old man with diabetes developed right foot necrotising fasciitis. He was referred to Wound Care Unit after wound debridement and Ray’s amputation of first and second toes. Upon presentation, initial wound assessment showed TIME:6.
He was started on ensymatic debridement gel for 3 weeks, followed by Aquacel Ag [ConvaTec] dressing for another 4 weeks. The dressing subsequently was changed to Deep-Seal [Zhejiang Longterm Medical Technology Co. Ltd] alginate wound dressing for the next 4 weeks.
In view of the poor progression of wound healing, KAdermin spray dressing was introduced. Wound healing improved gradually with marked reduction of area seen after 12 weeks on KAdermin spray [Figure 1].
Case 2
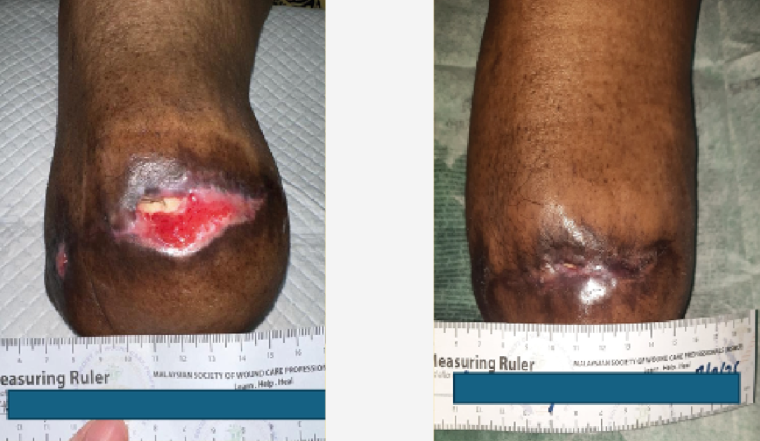
A 43-year-old woman with diabetes, hypertension and dyslipidemia presented to Wound Care Unit after extensive wound debridement of left foot. Initial wound assessment showed TIME:6. Desloughing and honey dressing were done once. Subsequently, dressing changes to silver dressing for 4 weeks duration. KAdermin spray was then introduced to the wound resulted with marked reduction in size after 12 weeks [Figure 2].
Case 3
A 33-year-old man with diabetes and hypertension presented after extensive wound debridement and Ray’s amputation of right big toe, second and third toes. Initial wound assessment showed TIME: 2. He was started on Aquacel Ag dressing. However, he developed infection after 8 weeks on Aquacel Ag and then underwent wound debridement.
Post-debridement, his wound was treated with KAdermin spray. There was a good response, with a reduction in wound size after 12 weeks of KAdermin spray dressing [Figure 3].
Case 4
A 53-year-old woman with diabetes and hypertension developed right foot necrotising fasciitis. She presented after wound debridement with initial wound assessment of TIME: 6. Wound dressing was done using Aquacel Ag for 4 weeks. Wound healing progression was slow and dressing changed to KAdermin spray. After 3 weeks of KAdermin spray dressing, there was marked improvement in healing with wound TIME:2. Her wound healed after 4 weeks of KAdermin spray dressing [Figure 4].
Case 5
A 53-year old man with diabetes, hypertension and dyslipidemia presented with chronic left DFU of the second toe exposing the distal phalange. The bone was nibbled and he was started on Aquacel Ag for 4 weeks. The dressing was then changed to KAdermin spray due to poor progression. His wound healed 4 weeks later [Figure 5].
Case 6
A 45-year old man with diabetes, hypertension and dyslipidemia developed right foot necrotising fasciitis. He presented after wound debridement with wound assessment of TIME: 6. After 8 weeks using Acticoat dressing, the wound improved to TIME:2. Then KAdermin spray was introduced to improve wound healing. The wound healed after 12 weeks of KAdermin use [Figure 6].
Results
The patients’ demographic data is shown in Table 1. Their wound progressions using KAdermin spray dressing is sumarised in Table 2. At 12 weeks or less, complete wound healing was observed in 30% of the patients, while another 70% of patients showed good responses with marked reduction in wound size. Wound healing was evidenced by the significant reduction in wound size and absence of infection during the period of wound dressing with KAdermin spray.
Discussion
The primary success of treatment using KAdermin dressing in DFU lies in its multi-dimensional approach. Traditional dressings often focus only on moisture or only on infection, while this combination addresses the three main barriers to diabetic wound healing.
The SCX complex (functionalised silicon dioxide with silver ions and chlorhexidine) offers broad-spectrum, sustained antimicrobial action, which is crucial for managing the chronic bacterial load and biofilm formation common in DFU (Afonso et al, 2021). Silver and chlorhexidine work together to break down bacterial biofilms that usually resist standard antibiotics. This anti-infective property is a significant advantage over simple dressings because managing infection is often the primary priority in DFU treatment.
A previous study by Pathi et al (2024) have shown that KAdermin dressing resulted in better efficacy in achieving faster wounds bacteria clearance and healing in infected wounds. In this study, wound bacteria clearance was observed in 86% participants in the KAdermin group versus 65.1% of those in the Mupirocin arm.
Hyaluronic acid is a vital component of the extracellular matrix and is often found at reduced levels in type 2 diabetic skin (Potekaev et al, 2021). Hyaluronic acid restarts the healing clock by signalling cells to migrate and repair, moving the wound out of the chronic phase. Hyaluronic acid in KAdermin dressing acts as a film-forming polymer that promotes tissue hydration and supports the natural processes of granulation and re-epithelialisation, which are often impaired in people with diabetes.
The kaolin in KAdermin spray has absorbent properties to manage excess exudate in wet wounds. This helps prevent maceration of the surrounding skin, while maintaining a moist wound healing environment (Huang et al, 2024). KAdermin dressing forms a physical barrier that protects the wound bed from external contamination, which is a significant risk for immunocompromised people with diabetes.
Our case study showed positive response rates from all patients despite the fact that five of the six patients had both diabetes and hypertension. This result is significant because patients with double comorbidities typically have very poor blood flow and much slower healing rates. A study by Zhou et al (2022) showed that diabetes is one of the most important which leading to a prolonged healing process and inferior clinical outcomes.
The fact that 30% reached full wound closure and 70% showed marked reduction in a high-risk group of patients suggests that this product’s combination of silver, chlorhexidine, silicon dioxide and hyaluronic acid is powerful enough to overcome poor vascular issue related to DFU.
Wound size reduction is a victory, even if the wound is not completely closed. By preventing infection, this combination treatment halts the progression toward gangrene. Reducing the wound size significantly within 12 weeks on KAdermin spray dressing moves the patient out of the high-risk category for amputation, which is the most critical clinical goal in DFU management.
Standard wound care often involves simple gause or basic antimicrobial creams which require frequent and painful changes. In our case study, a spray-based KAdermin dressing were used for wound dressing causes less trauma to the new tissue growing at the wound bed. At the same time, the Silicon Dioxide creates a protective shield that allows the Hyaluronic Acid to work undisturbed.
Limitations
Despite the encouraging clinical observations, several critical limitations must be considered when interpreting these results. Primarily, the small sample size (n=6) and the use of convenient sampling do not provide sufficient statistical power to make generalised conclusions regarding the efficacy of the spray. Furthermore, there was significant variability in patient demographics and initial wound presentations, including differences in wound surface area, depth and duration before the intervention. It is difficult to establish a standardised baseline because each patient presented with a unique clinical profile and varying comorbidities.
The lack of a control group further limits this study because it prevents a direct comparison between the KAdermin spray and standard care protocols. It is also important to note that patients had undergone various prior treatments, which may have influenced the wound bed’s readiness to heal. Although the 12-week observation period was sufficient for observing size reduction, it does not account for long-term tissue stability or recurrence rates.
Conclusion
The results of this case series suggest that the combination of silver, chlorhexidine, silicon dioxide and hyaluronic acid may provide a beneficial environment for managing the complex healing requirements of DFU. By addressing microbial load while simultaneously promoting tissue hydration, this multi-action approach showed a positive trend in wound size reduction across the observed cases. However, the preliminary nature of these findings must be emphasised. The significant variability in patient demographics and the diverse range of initial wound sizes coupled with the small sample size (n=6) preclude the ability to draw definitive statistical conclusions or generalise these results to the broader diabetic population. Furthermore, without a controlled comparative group, it is difficult to isolate the efficacy of the spray from the natural healing process or prior treatments. While these clinical observations are encouraging, they serve primarily as a foundation for more rigorous investigation. Large-scale, randomised controlled trials are essential to statistically validate the effectiveness of this treatment and to determine its impact across standardised wound classifications and patient profiles.
Ethical consideration
The case study has been registered with the National Medical Research Register (NMRR) of the Ministry of Health Malaysia (NMRR ID-25-03729-SI7).
Acknowledgements
The authors thank the Director General of Health Malaysia for his permission to publish this article.
Consent
Written informed consent was obtained from the patients for publication of this case study and accompanying images.