Chronic wounds (diabetic, venous, arterial, pressure and traumatic) impose substantial morbidity, costs, and carry risk of infection. Serial, effective debridement is a cornerstone of wound healing treatment (Wilcox et al, 2013).
Er:YAG laser debridement is an emerging modality for chronic wound management. By combining precise tissue removal with lower procedural pain, durable bioburden reduction, and pro-healing effects, it may serve as a valuable alternative to sharp debridement in selected patients (Hajhosseini et al, 2020).
The Er:YAG (2,940 nm) laser enables precise, superficial tissue ablation due to water‑peak absorption, allowing rapid removal of devitalised tissue and biofilm with minimal collateral thermal damage (Kaufmann and Hibst, 1996).
Short Erbium laser pulses generate mechanical stress waves; with RecoSMA (spatially modulated ablation), micro‑ablation areas induce deeper acoustic waves that may enhance microcirculation and trigger reparative pathways (Alcolea et al, 2017; Trelles and Khomchenko, 2019).
Recent evidence supports this approach: a prospective RCT (n=144) reported significantly higher complete epithelialisation by day 30 versus sharp debridement, with improved cleansing and granulation (Zaitsev and Asanov, 2025). Similarly, authors of single‑arm and prospective series in diabetic ulcers report consistent wound‑area reduction and healing with acceptable tolerance (Chilgar and Andurkar, 2023).
Methods
Study design and setting
This is a prospective single‑centre consecutive case series carried out at the Specialist Clinic Ambulatory Care Centre (SCACC), Hospital Kuala Lumpur, Malaysia. Seven adult patients with chronic, hard‑to‑heal wounds of mixed aetiology (diabetic foot ulcers, venous ulcers and traumatic wounds) were enrolled.
Ethics and consent
All patients gave written consent for treatment and for the use of de‑identified clinical data and photographs. As an observational service evaluation, formal Institutional Ethics Committee approval was not required as per local policy.
Inclusion and exclusion criteria
Inclusion criteria:
- Chronic wound ≥4 weeks’ duration refractory to standard treatment.
- Adequate vascular status as assessed clinically for local therapy.
- Ability to attend weekly follow‑up.
Exclusion criteria:
- Clinical signs of uncontrolled infection requiring systemic antibiotics or theatre debridement.
- Gangrene, deep compartment involvement not amenable to local laser treatment.
- Inability to consent.
Laser protocol
The study utilised the Multiline Er:YAG laser system (LINLINE Medical Systems, Belarus) equipped with the RecoSMA module [Figure 1]. RecoSMA (Reconstructed Spatially Modulated Ablation) is a proprietary technology that delivers spatially distributed micro-ablative laser pulses, creating controlled microscopic treatment zones while preserving intervening tissue.
Subjects received a two‑step Er:YAG protocol at each weekly visit:
- Ablative debridement: superficial vaporisation of necrotic debris to a clean, bleeding bed under visual control (typical ranges: ~10–15 J/cm², 1–10 Hz; tip 4–6 mm; energy reduced when approaching viable tissue).
- RecoSMA stimulation: spatially modulated Er:YAG to the wound bed and 3–5 cm periwound to induce acoustic micro‑injury and biostimulation (typical ranges: ~2–4 J/cm², ~3 Hz).
Smoke evacuation was used throughout (JUMBO Filtertrolley, ULT AG, Germany). No anaesthesia was required.
The parameter ranges applied were consistent with those specified in the device user manual (LINLINE Multiline, Er:YAG with SMA module).
Adjunctive care
- Cleansing with saline; appropriate dressings (e.g. silver alginate, HydroCyn gel, Kaltostat) were selected according to exudate/bioburden.
- Compression for venous ulcers as indicated.
- Offloading for plantar diabetic foot ulcers, with patient education on pressure avoidance and footwear.
Outcomes and assessments
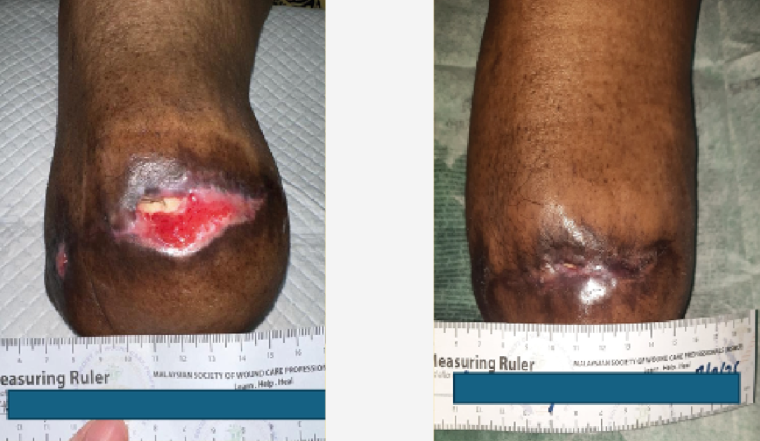
Primary outcomes were complete epithelialisation and percentage wound‑area reduction relative to baseline. Secondary outcomes were procedural tolerance, pain during debridement and inter‑session dressing changes. Wound area was measured by ruler and serial standardised photographs were taken at each visit. Adverse events were recorded.
Results
Seven patients were treated with weekly sessions (ablative + RecoSMA). All tolerated the procedures without anaesthesia; no adverse events were recorded. Cases demonstrated rapid conversion to a clean wound bed after ablation and visible granulation with serial RecoSMA. Progressive area reduction was documented week by week. Several wounds healed completely during follow‑up (cases 1, 2, 3 and 6). Other wounds reduced in size (cases 4, 5 and 7); however, these patients discontinued participation due to circumstances unrelated to the study protocol. Patient 3 did not attend treatments from week 9 through week 16 owing to hospitalisation unrelated to the diabetic foot ulcer. Patient 6 missed one session in week 4.
The case series summary is outlined in Figure 2, with the details of the individual patients shown in Figures 3–9.
Discussion
This consecutive series shows that Er:YAG ablation followed by RecoSMA stimulation is a practical, well‑tolerated adjunct for chronic wound care in an ambulatory setting.
These findings reflect the literature: a large randomised controlled trial demonstrated more frequent complete epithelialisation and faster cleansing/granulation with laser therapy versus sharp debridement by day 30 (Zaitsev and Asanov, 2025). Prospective series in chronic ulcers report consistent reductions in wound size and acceptable safety profiles (Alcolea et al, 2017; Chilgar and Andurkar, 2023).
The high water absorption coefficient of Er:YAG allows precise superficial ablation and effective biofilm disruption while minimizing thermal injury, while spatially modulated acoustic waves may enhance microcirculation and matrix remodelling up to several mm in depth. Strengths include a standardised two‑step protocol and real‑world outpatient feasibility without anaesthesia.
It should be noted that erbium laser ablation cannot completely replace sharp debridement, since in the case of large volumes of necrotic tissue, it is desirable to remove these mechanically because laser removal can take quite a long time.
Laser therapy should be viewed as an adjunct to, rather than a replacement for, standard wound-care practices. Its effectiveness is contingent on a comprehensive treatment approach, including compression therapy for venous ulcers, offloading for diabetic foot ulcers, and appropriate dressing strategies. Therefore, outcomes depend not only on laser application, but also on the quality and consistency of these concomitant measures.
For example, in Case 4 [Figure 6], new ulcers developed proximal to the original lesion during the treatment period. This may reflect deterioration in the patient’s general condition because of her age (87 years old), but could also have been influenced by concurrent therapies, dressings or other external factors.
Such observations highlight the need to interpret case-series findings with caution and to evaluate laser protocols within the full context of multidisciplinary wound management.
An additional observation concerned the management of wound edges. When moisture balance is not adequately controlled, edge maceration may develop, which can delay healing. In such circumstances, sharp debridement of compromised edges is often necessary to re-activate marginal epithelialisation. Case 7 provides a clear example: while the lateral wound healed more rapidly, the plantar wound progressed more slowly under otherwise similar conditions. This difference may be attributable to insufficient attention to edge management or suboptimal dressing choice. These findings highlight the importance of meticulous wound-edge care as a critical adjunct to laser treatment.
Limitations of this study include the small sample size, heterogeneity of aetiologies and incomplete quantitative datasets in this report. Future work should incorporate digital planimetry, pain scales, bacteriology where available and predefined endpoints to enable pooled analyses.
Conclusion
In seven consecutive chronic wounds of mixed aetiology, weekly Er:YAG debridement plus RecoSMA stimulation was feasible, painless for patients, and associated with progressive wound‑area reduction and healing. These observations support further controlled evaluation and protocol standardisation in multidisciplinary care.