Burn injury is a common worldwide problem: the World Health Organisation has stated that burns are the cause of approximately 180,000 deaths per year, with 11 million people experiencing burn injury annually (Radzikowska-Büchner et al, 2023).
It has been estimated that almost half of all global burn cases occurred in Asia in 2019, with the highest numbers of recorded burn injuries documented in China and India (Collier et al, 2022). Limited access to care and economic challenges have resulted in significant difficulties in delivering burn wound management in the region (Collier et al, 2022).
It must be noted that burn injuries can result in a profound and enduring psychological and social impact, which may extend well beyond the initial physical trauma. Common psychological concerns include post-traumatic stress, anxiety, depression and disruptions to self-perception. Caregivers may also be affected, often experiencing emotional fatigue and psychological strain, particularly when access to support services is limited (Dmitry et al, 2025).
To tackle this problem, the APAC Burns Peer-To-Peer Network was founded as a regional network of burn specialists, with the initiative to consolidate expert opinions on burn wound management and translate related clinical evidence into practice and implementation.
During the first consensus meeting, participants identified key factors in the successful assessment and treatment of burn wounds. This discussion and subsequent publication aimed to identify opportunities to improve the quality of burn wound care delivery, including standardising protocols, benchmarking outcomes and implementing best practices (Puri et al, 2025).
The publication also listed a number of recommendations for local practice that the expert panel reached consensus on, aimed at providing actionable steps for clinicians to improve burn wound management outcomes (Puri et al, 2025).
- Development of treatment guidelines for dedicated burn units and the standardisation of burn wound management protocols
- Training of district surgeons in primary first aid for burn wounds and burn wound management to enable specialist centres to focus on more complex cases and reduce the burden on referral systems
- Implementation of standard outcome measurements
- Motivating the medical community to advocate for resource allocation to burn care services, urging policymakers in respective countries to prioritise funding and infrastructure development for burn management.
Reflections since the previous consensus meeting
It was agreed that the published proceedings of the first consensus meeting (Puri et al, 2025) represented a successful start and provided helpful guidance, grounded in the panel’s clinical knowledge and experience, as well as the most up-to-date evidence.
At the follow-up consensus meeting, the panel shared case examples demonstrating how the previous publication has positively influenced their practice, leading to better patient outcomes, such as improved wound irrigation regimens (encompassing treatment rationale, technique and product choice) and dressing choices aligned with the guidelines.
The panel emphasised that disseminating this knowledge is crucial for standardising burn care and engaging healthcare providers across the region, ultimately improving patient access to best practices. See Box 1 for a summary of the dissemination framework.
The importance of standardised care
The panel identified that a key factor in reducing unwarranted variation in the assessment and treatment of wounds is the implementation of patient-focused care initiatives through clinical pathways (Adderley et al, 2017).
While there is no universal solution to reducing or removing variation in clinical practice, greater standardisation should be led by structured guidelines and pathways to focus wound assessment and management (World Union of Wound Healing Societies, 2020). This includes an accurate and thorough appraisal of wounds and a holistic assessment of individual patients, triggering appropriate care pathways that include ongoing monitoring and documentation. After stopping the burning process, wound bed preparation (WBP) should be seen as the starting point and underpinning of treatment.
Holistic care
The importance of holistic care was emphasised, considering the ‘whole’ patient, their overall health and circumstances and support network, as well as the wound itself. This particularly applies to burns, which are complex wounds encompassing a range of health-related factors. For example, patients with severe burns require metabolic and nutritional support to promote optimal healing (Jeschke et al, 2020).
It was noted that, in burn management, the goals of treatment go beyond wound healing and encompass restoring function so the patient can resume daily activities and reintegrate into society. For patients with burns, individual concerns such as cosmetic appearance (i.e. scarring) and the psychological impact of the trauma may be a priority in care. Maintaining mobility and promoting functional ability may also be key considerations.
When considering access to care, it has been shown that cultural, socioeconomic and geographic barriers often compound the psychological and social issues experienced by patients and their families, particularly in under-resourced populations (Dmitry et al, 2025).
All team members must deliver empathetic, person-centred care, enabling informed, collaborative decision-making and a strong focus on giving patients and their families a voice throughout the process.
Pain
Burns often cause patients to experience intense pain, with burn injury-induced pain having both inflammatory and neuropathic components. In severe burn wounds, the pain usually persists even after complete wound healing and hospital discharge, causing both long-term disability and neurological dysfunction (You et al, 2025).
Although pain is a key issue in burn injuries, its management generally remains suboptimal. The panel once again emphasised that it is vital to minimise pain during dressing changes. Pain during dressing changes can have both physiological and psychological impacts on the patient, and fear of dressing changes can significantly reduce quality of life (Lee et al, 2024).
All clinicians must listen to the patient’s perspective and consider the patient the expert on their own body and experience, particularly when assessing pain using validated assessment scales. Treatment decisions and product selection should be made with minimising pain at the forefront. It was noted that minimising pain during dressing changes can have lasting implications for patients’ quality of life even after their wounds have healed.
Treatment options in practice
Developing means to create greater access to advanced products and dressings was recognised as a priority. Increased awareness and education about the evidence and benefits of advanced product use aim to encourage healthcare providers to prioritise appropriate product selection.
Products and dressings for the management of burn wounds were discussed, with a focus on cleansing options and dressing selection. Wound irrigation with a solution was recommended, with the choice of specific cleansing agent dependent on the patient and their wound, balancing efficacy with potential cytotoxicity.
Burns are wounds that carry a high infection risk, particularly in severe or extensive burns, which are susceptible to serious complications, such as sepsis. In contrast, bacterial contamination of the burn wound itself can lead to biofilm formation, prolonging treatment and delaying wound healing (Markiewicz-Gospodarek et al, 2022).
Factors identified as contributing to the ‘ideal’ dressing for burn wounds were:
- Pain-free removal
- Ease of application
- Ability to remain in situ for several days (increased wear time)
- Ability to absorb exudate
- Ability to provide an antimicrobial barrier
- Ability to create a moist wound environment
- Cost-effectiveness.
Silver sulfadiazine
Use of silver sulfadiazine (SSD) dressings was discussed, as SSD has historically been a standard treatment for burn wounds. However, with evidence now available to support more up-to-date, advanced options, it has been recognised that SSD may have limitations and potential drawbacks, such as delayed wound healing, cytotoxicity and concerns regarding
its contribution to antimicrobial resistance
(Du et al, 2026).
Although SSD has been considered an economical choice, it is also associated with complications such as pain and increased risk of infection due to frequent dressing changes (Wasiak et al, 2013; Iswati et al, 2025). The panel agreed that, when selecting a dressing, consideration should be given to the total cost of treatment, bearing in mind that complications may prolong treatment and increase costs. Product choice often represents only a relatively small proportion of overall costs. Therefore, the cheapest dressing option may not be the most economical in practice.
With alternative options now available that offer comparable or superior outcomes without these drawbacks, healthcare providers should transition away from SSD and adopt alternatives to ensure the best possible care for patients. The panel agreed that silver-containing dressings provide a suitable alternative to SSD.
Silver-containing dressings
The panel agreed that silver-containing dressings, which can stay longer on the wound without changing the dressing, are a more effective alternative to SSD and significantly reduce the rate of wound infection. Silver-containing dressings have been found to be as effective as the standard of care (i.e. SSD), demonstrating additional benefits of decreased pain, lower hospital discharge time and lower treatment costs (Silverstein et al, 2011).
The panel recommended an approach based on the principles of undisturbed wound healing (UWH), selecting dressings that can be left on the wound for a number of days.
Wound irrigation solution
The panel recommended a wound irrigation solution with low concentrations of hypochlorous acid (HOCI) and sodium hypochlorite (NaOCI), which provides effective cleansing without cytotoxicity (Tsai et al, 2024).
The panel acknowledged that many other wound cleansing solutions are often used in practice – including common options such as tap water or saline solution, plus other commerically available cleansing products containing topical antimicrobial agents. It should be noted that any cleansing is better than no cleansing, particularly when there may be limited resources available.
However, the panel agreed that cleansing solutions incorporating HOCl/NaOCl have a strong evidence base for broad-spectrum efficacy balanced with patient safety, facilitating the mechanical removal of microorganisms and cell debris.
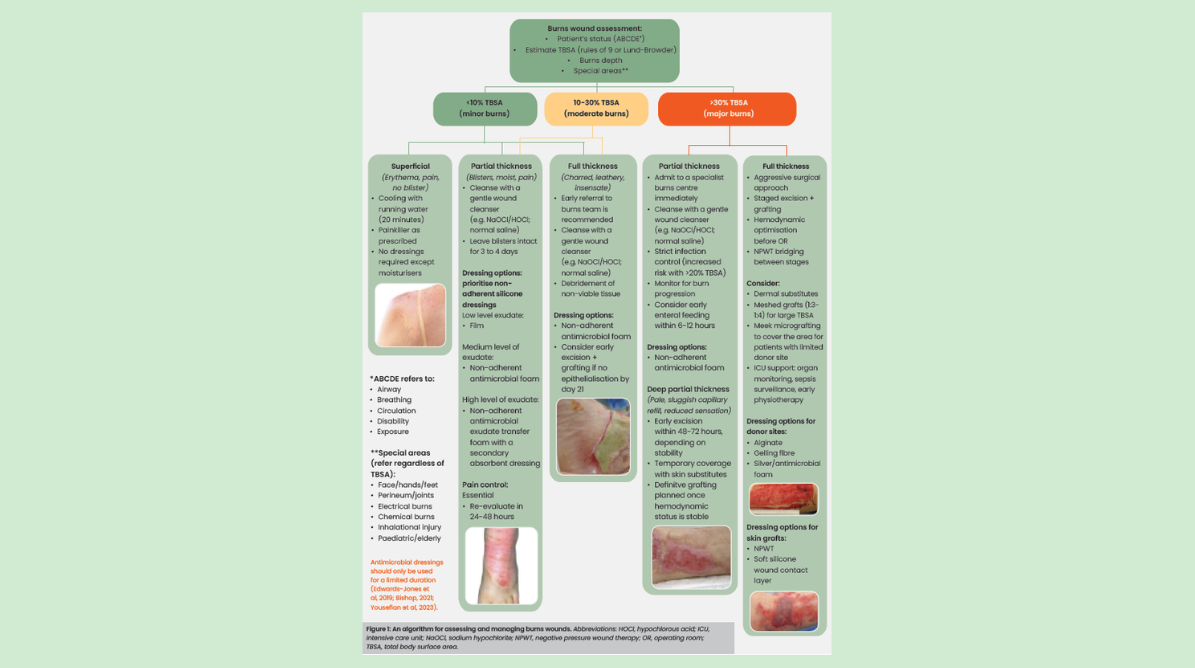
Algorithm for assessment and management
The panel developed an algorithm for assessing and managing burn wounds [Figure 1]. The algorithm aims to support standardisation of burn care and is based on total body surface area (TBSA) and burn type. It aims to provide comprehensive wound and pain management recommendations as per burn severity. Recommendations for when to make a referral are also outlined.
Increasing knowledge
It was agreed that publication of the first consensus document represented a successful start and laid the groundwork for educating clinicians across the APAC region. To standardise practice and optimise patient outcomes, increased awareness and knowledge are required, disseminating this ethos to as many healthcare providers across the area as possible.
Communicating evidence at a high level (e.g. government departments and authorities) is essential to instigating change; however, it is also vital to reach clinicians on the ground at all levels, including non-specialists. Separate guidelines tailored to different care settings and geographical regions may also be required. As well as standardising care for specialists, it is vital to ‘reach the unreached’ to harmonise understanding on a broader level, driving adoption across more diverse healthcare settings. Use of technology (e.g. mobile phones, apps, online platforms) can help make information widely accessible to all, potentially aiding the adoption of guidelines across geographical areas and skill levels.
Outcome measures
Measuring and tracking outcomes is a key part of the plan to add to the evidence base and raise knowledge and awareness. This will allow healthcare providers to make the case for the use of advanced products that have been shown to work effectively in practice.
Monitoring and documenting treatment and progress at every stage is vital to best practice. The following factors were identified as useful outcome markers to be tracked and documented in practice:
- Time to complete wound healing
- Patient satisfaction scoring
- Pain assessments (particularly during and after dressing changes)
- Scar assessment scoring
- Patients’ psychological and social recovery
- Predictive indicators of mortality.
Conclusions and next steps
Current evidence — along with the panel’s experience in practice — emphasises the importance of standardised care to reduce variations in practice and optimise patient outcomes. Despite the high prevalence of burns in the APAC region, there is a lack of standardisation and awareness of best practice.
The aim of this meeting report, following the first consensus document, is to educate clinicians at all levels and across the APAC region to adopt best practice for the care of patients with burns. This publication has provided an algorithm of care, based on the panel’s recommendations.