Burn injury is a common worldwide problem, with almost half of all global burn cases in 2019 occurring in Asia, and the highest numbers of recorded burn injuries documented in China and India (Collier et al, 2022). The World Health Organisation has stated that burns are the cause of approximately 180,000 annual deaths, with 11 million people experiencing some burn injury annually (Radzikowska-Büchner et al, 2023).
Burn injuries can be highly distressing for patients, challenging for caregivers and healthcare professionals (HCPs) and costly for healthcare systems. Burns often result in a profound and enduring impact on the patient, which may include common psychological concerns such as post-traumatic stress, anxiety, depression and disruptions to self-perception (Dmitry et al, 2025). Therefore, to minimise complications, it is important for HCPs to understand burns and their management, and have access to evidence-informed treatment methods.
Causes and classification of burns
Burns are wounds resulting from damage to the skin and other tissues (Zwierello et al, 2023), caused by the following factors:
- Heat (e.g. scalds from hot liquids, contact burns from hot solids, or flames)
- Radiation
- Electricity
- Friction
- Chemicals.
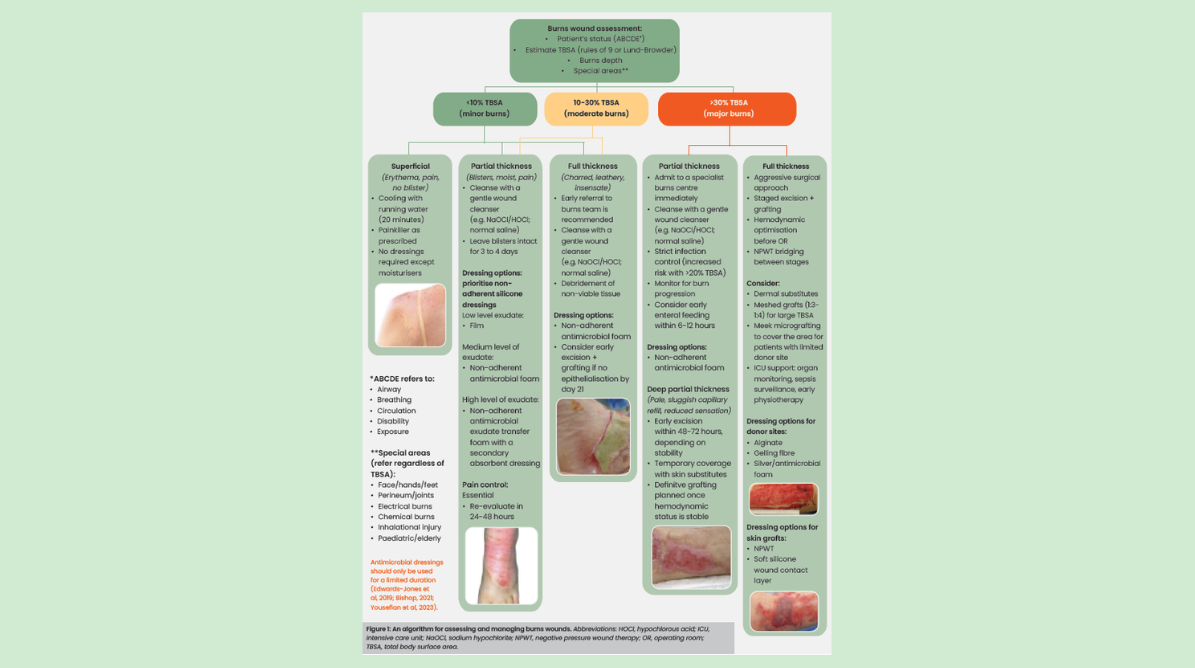
The severity of a burn determines the clinical care required. Burn severity varies widely and depends on factors such as anatomical site, temperature, duration of exposure, total surface area affected and depth (Evans et al, 2010). Burns are classified by their depth, with the increasing depth indicating greater tissue damage, which may lead to delayed healing and increased complications (see Figure 1 for burn classification; Zwierello et al, 2023; Malhotra et al, 2024). Accurate burn classification is important for selecting appropriate management. Otherwise, complications such as infection, scarring and contractures can significantly reduce the patient’s quality of life.
Challenges in managing burns
Managing burns is a complex challenge, often requiring multidisciplinary and specialised wound care, placing a significant burden on HCPs and healthcare systems globally. The overall aim of burn care is to minimise the adverse effects caused by the injury, contracture development, scarring and the impact on patient’s physical and emotional quality of life, while maintaining range of movement (Manasyan et al, 2025).
The burden associated with burn wounds, along with associated regional factors, such as limited access to care and financial constraints, has created substantial challenges for burn wound management across the APAC region (Puri et al, 2025). It is, therefore, important for HCPs to understand, and have access to, burn management tools that are easy to use and can be employed across diverse clinical settings.
Role of dressings in burn management
Topically applied products, such as creams and dressings, are minimally invasive burn management tools, providing a protective barrier and promoting wound healing. Expert consensus (Puri et al, 2025) and HCP experience (Nischwitz, 2021) broadly agree on the characteristics of an ideal dressing for management of burns in practice:
- Pain-free removal
- Easy application
- Ability to remain in situ for several days (undisturbed wound healing)
- Ability to absorb exudate
- Ability to provide an antimicrobial barrier
- Ability to create a sterile, moist wound environment
- Cost-effectiveness.
Traditionally, silver sulphadiazine (SSD) creams have been used as a standard treatment for partial-thickness burns (Hermans, 2019). However, side effects of SSD include leukopenia, hypersensitivity, allergic reactions, wound bed discolouration, antimicrobial resistance and pain during application and removal (White and Cooper, 2005; National Library of Medicine, 2023). Consequently, alternative approaches to the topical management of burns that are at least as effective as SSD, but associated with fewer side effects, should be considered (Davies et al, 2017). HCPs have access to a wide array of dressing types for use in burn care, including variants containing antimicrobial agents (e.g. silver) for when topical antimicrobial therapy is indicated. One such dressing is Mepilex Ag®.
Introducing Mepilex Ag dressings with Safetac® technology
Mepilex Ag (Mölnlycke Health Care) is a silver-containing absorbent foam dressing with Safetac technology. It is suitable for burn wounds, fulfilling the ideal dressing characteristics highlighted above. Mepilex Ag can be used for a wide range of wound types due to its gentle adherence, ease of application and removal and exudate absorption capacity; it may be used as an antimicrobial barrier to support the treatment of wounds when topical antimicrobial therapy is indicated (Puri et al, 2025). Additionally, Mepilex Ag has a wear time of 7 days (depending on the nature and condition of the wound). This longer wear time promotes undisturbed wound healing, which can improve burn wound outcomes.
Dressings with conventional adhesives may damage delicate wound tissue or fragile peri-wound skin (Charlesworth et al, 2014; Matsumura et al, 2014). It is important that HCPs are aware of and use dressings that reduce or even prevent dressing-related trauma (Puri et al, 2025).
Safetac is a technology based on soft silicone which can adhere to intact dry skin and remain in place on moist wounds or damaged surrounding skin without adhering to these fragile tissues (Cutting, 2008). Therefore, dressings with Safetac technology (e.g. Mepilex Ag) can be applied and removed without damaging the wound or stripping the epidermis of the surrounding skin (Cutting, 2008). The gentle yet effective seal formed between intact skin and a Safetac dressing helps limit the spread of exudate into surrounding tissue; this effect reduces the risk of moisture-related peri-wound damage (e.g. maceration). By reducing trauma to the wound and peri-wound area during removal, Safetac dressings help minimise pain during dressing changes. Numerous studies in healthy volunteers (Dykes et al, 2001; Dykes, 2007; Waring et al, 2008; Waring et al, 2011) and in patients with chronic wounds (Zillmer et al, 2006) have shown that dressings with Safetac are less traumatic to remove than dressings that use other adhesive systems.
Clinical evidence for Mepilex Ag
Table 1 provides a summary of randomised clinical trials comparing Mepilex Ag with a variety of other interventions and SSD, highlighting the better outcomes achieved with Mepilex Ag (i.e. reduced healing time and dressing-related pain, better scar outcomes, higher patient and clinician satisfaction and lower treatment costs).
Case studies
Case studies advance clinical knowledge and can help demonstrate the scale of clinical problem, the intervention required and its impact on outcomes (Piker, 2026). See pages 4 and 5 for case studies demonstrating the positive outcomes achieved with Mepilex Ag in patients with partial-thickness burns.
Conclusion
It is recommended to use burn wound dressings that minimise pain and infection risk, prevent trauma to the wound and peri-wound skin, improve ease of use for HCPs and reduce overall care costs for healthcare systems (Puri et al, 2025). The clinical evidence and case studies presented in this Made Easy highlight the effectiveness of Mepilex Ag in achieving these outcomes in both adult and paediatric patients.
Download the PDF below to access the full Made Easy resource.